








Hip arthroscopy
Hip arthroscopy is a minimally-invasive technique (key-hole surgery) by which the orthopaedic surgeon can inspect the interior of the acetabulofemoral (hip) joint and treat several pathological conditions. This surgery is done by making small cuts around the hip, inserting a tiny camera (arthroscope) for viewing, and other slim instruments to perform several procedures. Unfortunately this method fell into disfavor by the orthopaedic community for many years, and the reason was the lack of specialized instruments and know-how, which rendered it a very difficult, almost impossible technique to perform.
If one observes a hip radiograph in detail, he will soon realize that inserting an instrument in the gap between the femoral head and the acetabulum (the two parts of the bones that form the hip joint) would be a very a painful, if possible, procedure to do. The reason is that the hip joint has a ball-and-socket shape and the first impression of an inexperienced observer is that, as there is no straight gap between the two bones, placing an instrument would be an impossible job to do. Furthermore, the hip joint is deeply situated, in contrast to the knee joint, and even the shoulder, and surrounded by a thick layer of muscles, tendons, capsule and synovium. This led Dr Burman, in 1931, to state that hip arthroscopy is impossible. This viewpoint was dominated the literature for many years.
Nowadays all these obstacles have been overcome with the use of thin, extra-long instruments, improved cameras, use of optimized patient position and adequate and safe distraction of the hip joint. Advances in instruments technology and techniques allowed easier arthroscopic access to the hip joint and accomplishment of effective procedures to deal with hip problems. This is the reason that hip arthroscopy is only undertaken by highly – specialized orthopaedic surgeons, as this surgical technique demands a long learning curve. Today, hip arthroscopy is an inextricable part of hip surgery and is helping patients in elimination of pain, increase of hip mobility and delay of a possible hip arthroplasty.
Hip arthroscopy is also described as a preservation surgery, as by this method the surgeon respects and preserves most of the structures of the native hip, and in some occasions tries to modify the structures in order to resemble more to the normal anatomy, especially in cases with congenital anomalies (different shape of the bones from childbirth). This renders the technique very different to hip arthroplasty, by which we resect all the pathological tissues and replace the whole joint with an artificial one.
In the early years of hip arthroscopy, one could use the technique just for diagnostic reasons. The surgeon would inspect the hip and could locate pathological conditions. At present, we can not only diagnose but also treat these conditions and carry out a number of surgical procedures.

Figure 1: The setup of theatre during a hip arthroscopy. The whole procedure is carried out through 3 small holes. The surgeon works with slim instruments while he can view the interior of the joint on the monitor.
A tear of the acetabular labrum is perhaps the most common cause of chronic hip pain. The acetabular labrum is a soft-tissue structure, which is the extension of the acetabular cartilage (gristle) of the acetabulum (socket). Its role is the enlargement of the acetabular surface and the “sealing” effect of the acetabulum onto the femoral head (ball). It plays a significant role in the hip biomechanics. Also, plays a protective role to the acetabular cartilage. This implies that an injury or tear to the acetabular labrum may endanger the cartilage, resulting in the further damage of the whole joint. Fortunately, an acetabular labral tear creates significant hip pain and, in some occasions, significant disability, and brings patient to the orthopaedic surgeon. With hip arthroscopy a labral repair may be done, either with smoothening, debridement or even repair with arthroscopic sutures.
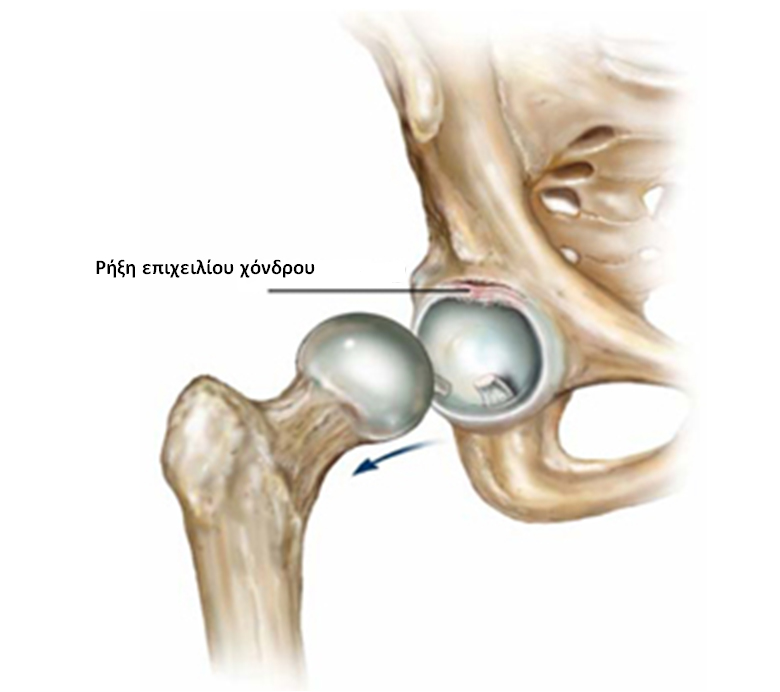
Figure 2: The acetabular labral tear is very commonly located at the anterior area (front of the labrum).
Femoroacetabular impingement is another cause of chronic hip pain. This condition could be described as the abnormal shape of either the femoral head (ball) or the margin of the acetabulum (socket), both of which have excessive bone. In the first case the impingement is called CAM, while in the second case PINCER-type impingement. Very frequently the two types of impingement coexist. Whichever it is, the result is the pinching of the acetabular labrum between the two bones in the extreme movements of the hip joint, which creates chronic hip pain, and may even cause a labral tear in the long run. The treatment of these two conditions is the removal of the excessive bone arthroscopically with special tools (burs) and reshaping the bones in order to resemble to the normal anatomy.
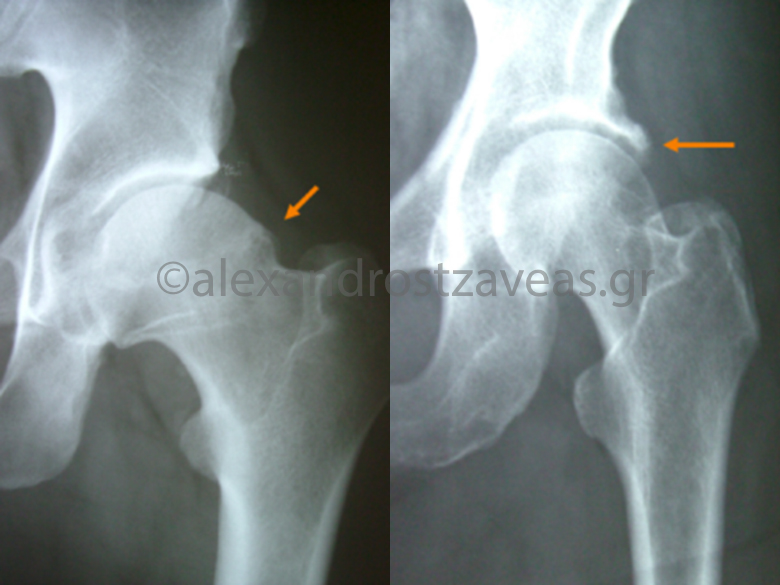
Figure 3: Femoroacetabular impingement is a common cause of chronic hip pain. The lesion may be localized either at the femoral head (left figure) or at the acetabular margin (right figure).
Many other conditions of chronic hip pain may be treated with hip arthroscopy, namely loose or foreign bodies, hip infection, chondral lesions, osteochondritis, early osteoarthritis, ligamentum teres injuries, synovitis, PVNS (pigmented villonodular synovitis), synovial chondromatosis, AVN (avascular necrosis of the femoral head), painful total hip replacement. Moreover, hip arthroscopy may address problems in the area around the hip joint, the so-called extra-articular pathology, like trochanteritis, Iliopsoas tendinitis, snapping hip, iliotibial band syndrome, sciatic nerve compression and ischiofemoral impingement.
Hip arthroscopy is an outpatient surgery, and only in some occasions patients may stay in the hospital for one night. Ιt is generally a pain-free operation. The procedure generally takes 1-3 hours to be performed and involves 2-3 small punctures at the lateral aspect of the hip. The patient can walk and do stairs the same day of the operation. Post-operatively patients should be under the care of a physiotherapist for a few weeks and a rehabilitation protocol is followed.

Figure 4: Representation of the portals through which the camera and other instruments are introduced into the hip joint.
Hip arthroscopy combines the advantages of a minimally-invasive, hip-preservation, outpatient procedure and opens up new horizons in the understanding, prevention and treatment of pathological conditions of the hip joint.


