








FAI (femoro – acetabular impingement)
The FAI (femoro – acetabular impingement) described long time ago, but only relatively recently has been associated with hip symptomatology and has been considered as etiological factor for degenerative changes in the joint. The FAI is the abnormal friction between the femoral head – neck junction and the acetabular rim. The condition may be either a result of the anatomical structure (excessive retroversion of the acetabulum, the low offset of femoral head) or the excessive range of motion (in people with strenuous physical activity).
Two distinct types of femoroacetabular impingement have been described. The pincer - type that occurs as a result of anterior acetabular overcovering or increased retroversion of acetabulum, and cam - type (femoral impingement due to hyperostosis) that occurs when there is loss of sphericity of the femoral head, which impinges to the front rim of the acetabulum, particularly during flexion and internal rotation of the hip, thus exerting repeated compression and shearing forces to the chondro – labral junction. The non-spherical femoral head created by structural abnormalities of offset, usually described as a pistol - grip deformity of the femoral neck. It is very common for pincer and cam – type impingement to coexist.
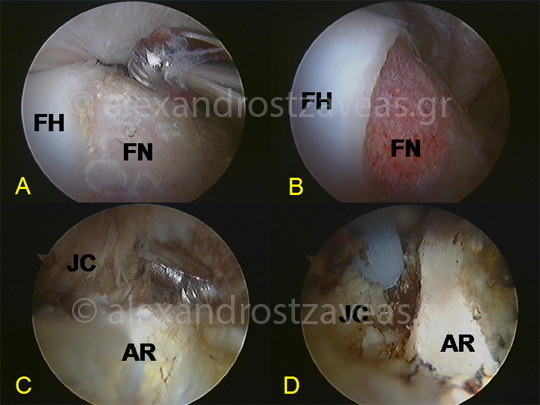
The arthroscopic treatment of impingement lesion. (A: femoral hyperostosis (CAM), B: restoration of normal anatomy after removal of the lesion, C: "pincer”-type lesion, D: image after acetabular recession (FH: femoral head, FN: femoral head – neck junction, JC: joint capsule, AR: acetabular rim)
The objective of the arthroscopic treatment is the removal of bone at the femoral head – neck junction for impingement cam - type and acetabular recession for pincer type impingement, which restores the normal hip mechanics, especially in extreme movements, and concurrent repair of the labrum. This results in the elimination of micro – injury at the anterior edge of the acetabulum, the disappearance of pain, and, potentially, the slowing down of the progression of osteoarthritis in young patients.


